

Abstract
Background: Relapse is a major challenge in treating patients with MDS and AML. In this study we used a genomics-informed computational biology modeling (CBM) technique to understand the mechanisms of relapse after chemotherapy treatment and to postulate new re-induction treatment options.
Methods: 120 patients with AML or MDS were recruited in the iCare1 prospective clinical study (NCT02435550), designed to assess predictive accuracy of CBM prediction by comparing computer predictions of treatment response to actual clinical outcomes. WES, CNV, and cytogenetics were obtained for 96 patients (Table). Genomic profiling was conducted by conventional cytogenetics, whole exome sequencing (SureSelectXT Clinical Research Exome, Agilent), and array CGH (Agilent). Somatic genomic mutations were inputted into CBM technology to create disease-specific protein network maps for each patient. A digital drug library of FDA-approved drugs was created for CBM by programming each agent's mechanism of action determined from published literature. Digital drug simulations of the patient's choice of therapy were tested at varying doses and predicted efficacy of the drugs were measured as a function of a disease inhibition score (DIS), defined as the degree to which disease pathways and phenotypes (cell proliferation and viability) were returned to a mutation-free state. Treating physicians were masked to the results of CBM predictions and the clinical outcomes were prospectively recorded. Clinical response for MDS patients was defined as CR+PR+HI (IWG 2006). Clinical response for AML patients was defined as CR+PR by IWG 2003 criteria.
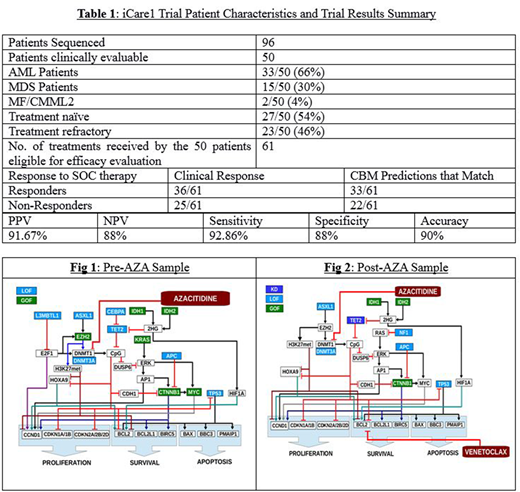
Results: 50 patients were eligible for evaluation based on length of follow-up. In 50 patients, 61 treatments were administered. CBM maps of relapsed samples from iCare 1 patients accurately matched the patient's nonresponse of treatment at relapse in 90% of patients and identified mechanisms for chemoresistance in these patients (Table 1).
An example case-study is presented (CASE I: UFH-00012): AML patient, relapsed after 7+3 induction therapy. CBM predicted response to azacitidine (AZA) at first relapse and clinically was evaluated to be a responder with a blast reduction to 2%, normal CBC, and normal cytogenetics. After 9 months of AZA, the disease relapsed and was genetically profiled. CBM analysis and digital drug simulation of the relapsed disease genomics confirmed a non-response to AZA. A GOF mutation in EZH2 present in pre-AZA was a key driver of response while this was missing in the AZA-refractory sample. ASXL1 mutation was present in both samples and without the EZH2 mutation in after-AZA sample is posited as the mechanism for AZA resistance. Digital drug screening identified the combination of AZA with venetoclax as a possibly effective drug combination due to upregulation of BCL2 in this patient's disease network. Simplistic network schematics derived from the CBM analysis for pre and post AZA samples are illustrated in Figs 1 & Fig 2.
Conclusions: Genomics-informed CBM accurately predicted response to standard of care in MDS and AML and identified mechanisms for induction failure. Loss of EZH2 mutation was identified as a possible mechanism for AZA-resistance in the face of ASXL1 mutation. CBM analysis of the refractory disease predicted a new therapy option for this patient based on the evolved disease characteristics.
Vali:Cell Works Group Inc.: Employment. Abbasi:Cell Works Group Inc.: Employment. Singh:Cellworks Research India Private Limited: Employment. Usmani:Cellworks Research India Private Limited: Employment. Lala:Cellworks Research India Private Limited: Employment. G:Cellworks Research India Private Limited: Employment. Radhakrishnan:Cellworks Research India Private Limited: Employment. Birajdar:Cellworks Research India Private Limited: Employment. Naga:Cellworks Research India Private Limited: Employment. Cogle:Celgene: Other: Steering Committee Member of Connect MDS/AML Registry.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal